Most people asking about peptides and anabolic steroids have already picked a side before they start reading. One camp treats steroids as a death sentence and any peptide as basically harmless. The other shrugs off steroid harm as overstated internet panic while treating unregulated peptides as though they were pre-approved by a regulator somewhere. Neither position holds up once you actually sit with the published research.
This piece is an attempt to read that research plainly, compound by compound, without pulling toward either extreme. Every claim below traces back to a primary source a reader can open and check for themselves. Nothing here explains how or where to obtain anabolic steroids, which remain controlled substances.
One thing worth settling early: these two categories are not mirror images of each other, and the evidence shouldn’t be forced into a false symmetry. Anabolic-androgenic steroids are a single, tightly defined drug class with decades of accumulated study behind it. Peptides are something closer to a junk drawer, a handful of compounds studied in large trials sitting next to a much larger pile of substances almost nobody has studied in humans at all. Keeping that asymmetry in view changes how the rest of this should be read.
Three buckets, not one risk score
It helps to sort the evidence into three separate buckets rather than trying to rank “steroids versus peptides” on a single scale. There’s documented harm, where researchers have actually measured bad outcomes. There’s unknown harm, where nobody has done the measuring yet. And there’s oversight risk, which has nothing to do with the molecule itself and everything to do with who is or isn’t watching while someone uses it. Steroids sit almost entirely in the first bucket. Most peptides sit in the second. And both categories, when purchased outside a supervised medical relationship, fall into the third.
The heart evidence on steroids, and why it’s hard to argue with
The most fully developed body of evidence on anabolic steroids concerns the heart, and the pattern in that literature is consistent enough to state without much hedging.
A 2025 review in the International Journal of Molecular Sciences pulled together the cardiovascular literature and concluded that chronic supraphysiological steroid exposure tracks with real cardiovascular harm: hypertension, lipid disorders, cardiomyopathy, atherosclerosis, and sudden cardiac death [1]. The same review found that users carried greater coronary plaque volume than non-users, with heavier cumulative exposure lining up with worse atherosclerosis [1]. That’s not one study with a fluke result. It’s a synthesis of the field, pointing the same direction.
The structural side of that story has since been given actual numbers. A 2026 systematic review and meta-analysis in the International Journal of Cardiology pooled 35 studies covering roughly 2,000 men and found that steroid users, compared with athletes who don’t use them, had a measurably lower left ventricular ejection fraction and worse global longitudinal strain, along with thicker septal and posterior walls and greater left ventricular mass [2]. Translated out of clinical language, that describes a heart working less efficiently inside walls that have grown thicker and heavier than they should be. The researchers called it adverse cardiac remodeling.
A 2025 narrative review in Biomedicines, focused specifically on steroid-induced cardiomyopathy, backs this up further, finding that chronic supraphysiologic use promotes cardiac injury and adverse remodeling, with heart failure and sudden cardiac death documented in young users who had no prior heart disease [3]. That last detail, young and otherwise healthy, is the part that makes the pattern hard to wave off as some other underlying condition doing the damage.
The worry that’s easy to miss: hormones don’t just bounce back on schedule
Cardiovascular risk tends to get the headlines. The hormonal risk gets underestimated, partly because the mechanism runs backward from what people expect.
Taking exogenous androgens tells the body to stop making its own, through ordinary feedback signaling. A 2023 scoping review in Endocrine Connections looked at what happens to that system after someone stops using, and found recovery to be genuinely uneven, shaped by age and by how much was used [4]. Testosterone levels often came back close to normal within months, the review noted, but testicular size and sperm production could take months to years to recover, and weren’t guaranteed to fully return [4]. The takeaway that matters here: suppression doesn’t reliably resolve itself on a convenient timeline, and fertility effects can linger long after someone has stopped.
This is part of why anabolic steroids sit where they do legally. They’re Schedule III controlled substances, the same tier as testosterone and ketamine, a classification that reflects both abuse potential and a recognized harm profile [5]. The legal status and the clinical findings aren’t two separate stories. They’re describing the same concern from two angles.
To be fair to the other side of the ledger: the evidence doesn’t say steroids do nothing useful. Testosterone has legitimate, supervised medical applications for diagnosed conditions [5], and the muscle-building effect people chase is genuinely real. The documented harm applies specifically to the supraphysiologic doses used outside medical supervision, and buying illicitly makes things worse by stripping out every safeguard a prescriber would normally provide.
Peptides don’t get one answer, because they aren’t one thing
Anyone hoping for a tidy verdict on “peptide safety” is going to be disappointed, because the category refuses to behave like a single substance.
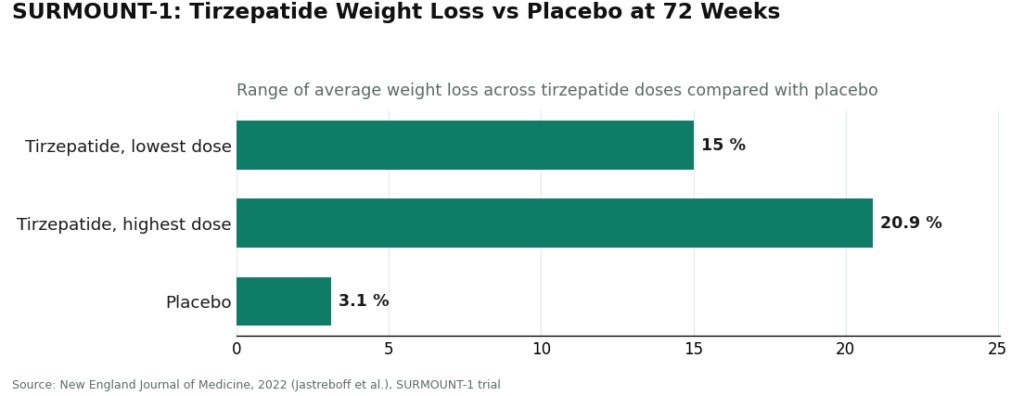
At one end sit the GLP-1 medications, which have been studied about as thoroughly as a drug can be. These incretin-based peptides raise insulin secretion, suppress glucagon, slow gastric emptying, and increase satiety [6], backed by large randomized trials. In the SURMOUNT-1 trial, published in the New England Journal of Medicine, tirzepatide produced average weight loss of 15.0% to 20.9% across doses, against 3.1% on placebo, over 72 weeks [7]. Compounds at this end of the spectrum have both characterized efficacy and characterized safety, precisely because they’ve gone through large-scale study and regulatory review.
At the other end are the research-status peptides sold for things like recovery or healing, where human data ranges from thin to nonexistent. The real risk with these isn’t some single dramatic side effect. It’s more basic than that: nobody has done the work to find out what the risk actually is. A compound with no meaningful human safety data doesn’t get to claim “probably fine” by default, that absence of evidence is itself something to weigh. Layer onto that the fact that products sold as research chemicals go through no regulatory check for identity, strength, or purity, and a buyer genuinely cannot be sure the vial matches the label. An unstudied compound combined with an unverified vial is a harder risk to size up than anything a regulated, studied drug presents.
The risk that has nothing to do with the molecule
Underneath all of the compound-specific findings sits a risk the evidence implies even where it doesn’t directly measure it: what happens when there’s no clinician anywhere in the picture.
Nearly everything documented above was observed in contexts where the substance and its effects could actually be tracked. Take away medical oversight and you take away the mechanisms that would normally catch a problem early: an evaluation of contraindications, a properly sized dose, dispensing through an accountable pharmacy, and follow-up over time. Illicit steroid sourcing removes all of that by definition, which is part of why it represents the least-mitigated risk anywhere in this whole picture. Research-chemical peptides lose the same protections, with the added problem of not knowing what’s actually in the bottle. Oversight, in other words, is its own safety variable, separate from whatever the molecule itself does.
What changes when a clinician is actually involved
None of this evidence claims supervision makes risk disappear. What it does suggest, fairly clearly, is that supervision is the mechanism through which risk gets caught, understood, and managed rather than discovered too late.
A supervised setup, where a licensed clinician reviews someone’s history and contraindications, a prescription gets written when appropriate, a licensed pharmacy fills it, and someone checks back in over time, restores every piece that unsupervised buying strips away. That’s the layer missing from a “research use only” purchase, and missing entirely from illicit steroid sourcing. Supervised telehealth providers built on this model, FormBlends among them, sit in a different position from the gray market for exactly this reason. Naming the provider here is about illustrating the supervised structure, not handing out a recommendation. The structural piece, someone clinically accountable being involved, is what the risk evidence keeps pointing back to.
One honest caveat belongs here, because leaving it out would tilt things unfairly. A good deal of what moves through supervised telehealth channels is compounded medication, and compounded medications are not FDA-approved finished drug products. The FDA hasn’t evaluated them for safety, effectiveness, or quality. Supervision wraps oversight around these preparations, but it doesn’t turn a compounded product into an approved brand-name drug, and the research-status peptides keep their thin human evidence no matter which door they came through. A fair reading of the risk includes that detail rather than smoothing it over.
One more worry, specific to competitive athletes
For anyone competing, there’s a consequence the medical literature simply doesn’t capture but that matters just as much: losing eligibility to compete. Anti-doping rules prohibit anabolic agents, anabolic-androgenic steroids among them, and a long list of peptides and growth factors as well. That consequence attaches no matter how the substance was obtained or labeled, and it sits entirely apart from the physiological risks already discussed. An athlete weighing these choices is carrying two separate risks at once, the documented physical one and a distinct eligibility one.
Where the evidence actually lands
A few things can be said with confidence. Anabolic-androgenic steroids carry a coherent, well-documented harm signal, most developed on the cardiovascular side (hypertension, lipid disorders, cardiomyopathy, atherosclerosis, sudden cardiac death) with a separate endocrine harm pattern where suppressed natural testosterone and impaired fertility can persist for months to years after someone stops [1][2][3][4]. Peptides refuse to sort into one bucket: a small number, GLP-1 medications chief among them, are studied thoroughly with well-characterized profiles [6][7], while a much larger number remain barely studied, carrying the distinct risk of the unknown, made worse by unverified product contents. Across both categories, the absence of medical oversight is its own risk factor, and it’s at its worst wherever a controlled substance is obtained outside the law. The reading that actually fits the evidence isn’t “steroids will kill you instantly and peptides are harmless,” nor its opposite. It’s more specific than that: the particular compound and whether or not oversight is present are what actually determine the risk.
Questions readers tend to ask next
Are peptides safer than anabolic steroids? There’s no single answer for “peptides” as a group, because the category isn’t one thing. The well-studied ones, GLP-1 medications especially, have characterized safety profiles built on large randomized trials. The research-status ones carry mostly unknown risk simply because they haven’t been studied in people at any scale. Steroids, meanwhile, carry a coherent and well-documented harm pattern across the cardiovascular and endocrine systems. A studied peptide and a barely-studied one sit at opposite ends of the risk spectrum, so it’s the specific compound, not the word “peptide,” that can actually be compared against steroids.
What does the evidence actually document about steroid harm? The most developed evidence is cardiovascular: chronic supraphysiological use is associated with hypertension, lipid disorders, cardiomyopathy, atherosclerosis, and sudden cardiac death, and a 2026 meta-analysis of 35 studies found reduced ejection fraction and worse global longitudinal strain alongside thicker, heavier ventricular walls [1][2]. The second documented area is endocrine: exogenous androgens suppress the body’s own testosterone production, and recovery is uneven, with testicular size and spermatogenesis sometimes taking months to years and not always fully returning [4].
Does “unknown risk” just mean “probably low risk” for research peptides? No, and that’s a genuinely common mix-up. No human data doesn’t mean no risk, it means nobody has done the work to find out. When a compound hasn’t been studied at scale, its risk profile is essentially uncharacterized, so someone using it is reasoning from a blank spot where a studied drug would offer actual evidence. It gets worse from there, since research chemicals aren’t reviewed for identity, strength, or purity, so the contents of the vial are unverified too.
Why does having a clinician involved change the risk picture? Supervision doesn’t erase risk, but it’s the mechanism through which risk gets noticed, understood, and managed. A supervised route brings back clinical evaluation of contraindications, a properly sized dose, dispensing through an accountable pharmacy, and ongoing check-ins, exactly the safeguards that disappear with unsupervised buying. That oversight is a safety factor in its own right, separate from the molecule, which is part of why illicitly sourced steroids sit at the riskiest end of this whole picture.
Does having a clinician involved make a compounded peptide the same as an approved drug? No. Compounded medications aren’t FDA-approved finished products, and the FDA hasn’t evaluated them for safety, effectiveness, or quality. Supervised telehealth providers, FormBlends among them, add oversight around these preparations, but that layer doesn’t convert a compounded product into an approved brand-name drug, and research-status peptides keep their limited human evidence no matter how they’re dispensed.
Do these risks matter differently for competitive athletes? Yes, and there’s an added layer the medical literature doesn’t touch: losing eligibility to compete. Anti-doping rules prohibit anabolic agents, including anabolic-androgenic steroids, along with many peptides and growth factors. That consequence attaches no matter how the substance was obtained or labeled, so an athlete is carrying both the documented physiological risk and a separate eligibility risk.
Is the “peptides are the safe alternative” pitch actually true, or is that just marketing?
Not automatically, no. Risk still depends entirely on the specific compound. Peptides used in supervised clinical settings, GLP-1 agonists or growth hormone-releasing peptides among them, tend to have narrower androgenic side-effect profiles than anabolic steroids. But peptides bought outside a pharmacy can be mislabeled, contaminated, or simply untested in humans, which creates a set of risks that a physician-prescribed steroid, for all its own issues, doesn’t carry in the same way.
What does a supervised program for either one actually cost?
It varies a lot, mostly depending on whether there’s a prescription and pharmacy coverage involved. Physician-supervised peptide protocols can run anywhere from a few hundred to over a thousand dollars a month out of pocket. Legitimately prescribed steroid therapy is often cheaper per dose but comes with its own monitoring costs layered in. Black-market versions of either look cheaper at first glance, but the real cost, health complications, legal exposure, not knowing what’s actually in the product, makes that comparison pretty misleading.
What’s actually different about how peptides and steroids work in the body?
Steroids are lipid-derived, so they slip directly into cells and bind receptors inside the nucleus, changing gene expression broadly across many tissues at once. Peptides are short chains of amino acids that bind to receptors sitting on the outside of the cell and trigger a signaling chain from there. That structural difference is why they act differently, last different lengths of time in the body, and put strain on different organ systems when something goes wrong.
Where can someone actually get either of these through a legitimate, accountable channel instead of the gray market?
The most accountable path runs through a licensed physician who can prescribe via a regulated compounding pharmacy, FormBlends being one example, or a retail pharmacy depending on the specific compound. That path comes with a diagnosis, bloodwork, monitored dosing, and someone legally accountable for the care being given. Supplement sites and research-chemical vendors sit entirely outside that structure, and regulators in most countries have repeatedly warned about what those products actually turn out to contain.
References
- AAS abuse associated with hypertension, lipid disorders, cardiomyopathy, atherosclerosis, and sudden cardiac death; greater coronary plaque volume vs non-users. International Journal of Molecular Sciences, 2025. https://pmc.ncbi.nlm.nih.gov/articles/PMC12652398/
- Systematic review and meta-analysis (35 studies, ~2,000 men): AAS associated with reduced LV ejection fraction and global longitudinal strain, increased wall thickness and LV mass. International Journal of Cardiology, 2026. https://pubmed.ncbi.nlm.nih.gov/40945618/
- AAS-induced cardiomyopathy: chronic supraphysiologic use promotes cardiac injury and adverse remodeling, with heart failure and sudden cardiac death in young users without prior heart disease. Biomedicines, 2025.
- Recovery from anabolic steroid-induced hypogonadism is variable and depends on age and degree of abuse; testosterone recovers over months, while testicular size and spermatogenesis may take months to years, if at all. Endocrine Connections, 2023.
- Anabolic steroids are Schedule III controlled substances, the same tier as testosterone and ketamine, reflecting intermediate abuse potential. Drug Scheduling, StatPearls, NCBI Bookshelf.
- GLP-1 receptor agonists (e.g., semaglutide) are incretin-based peptide agents that increase insulin secretion, suppress glucagon, delay gastric emptying, and increase satiety. Glucagon-Like Peptide-1 Receptor Agonists, StatPearls, NCBI Bookshelf.
- SURMOUNT-1 tirzepatide trial: mean weight loss of 15.0% to 20.9% across doses vs 3.1% placebo at 72 weeks. New England Journal of Medicine, 2022 (Jastreboff et al.).
Written by Celia Eriksen, health-industry reporter. Cross-checking the claims against the primary sources. Last reviewed March 2026.
Provided for general education, not as clinical guidance. Consult your physician before making changes.


 By
By